Black Women: Bearing the Greatest Burden
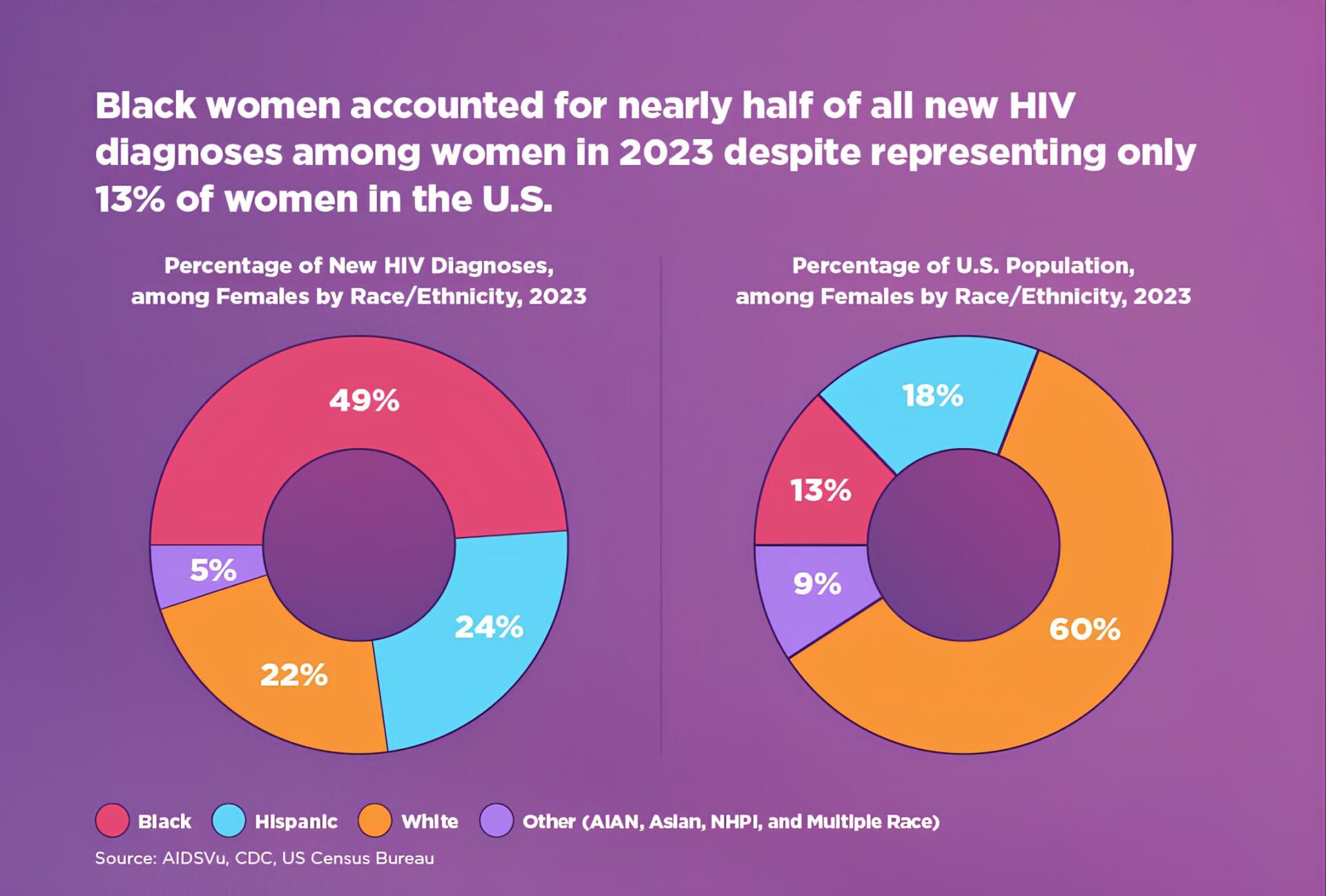
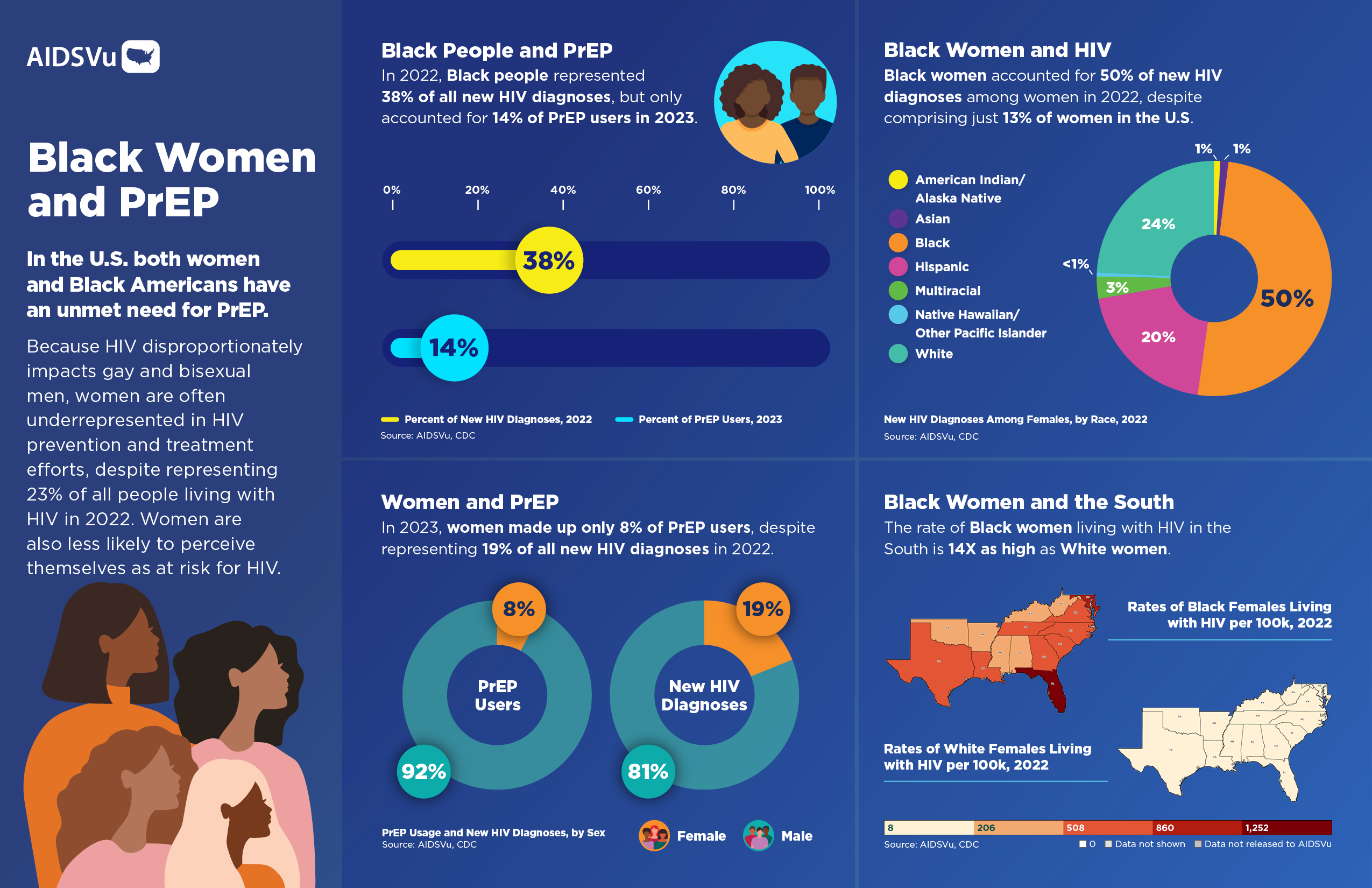
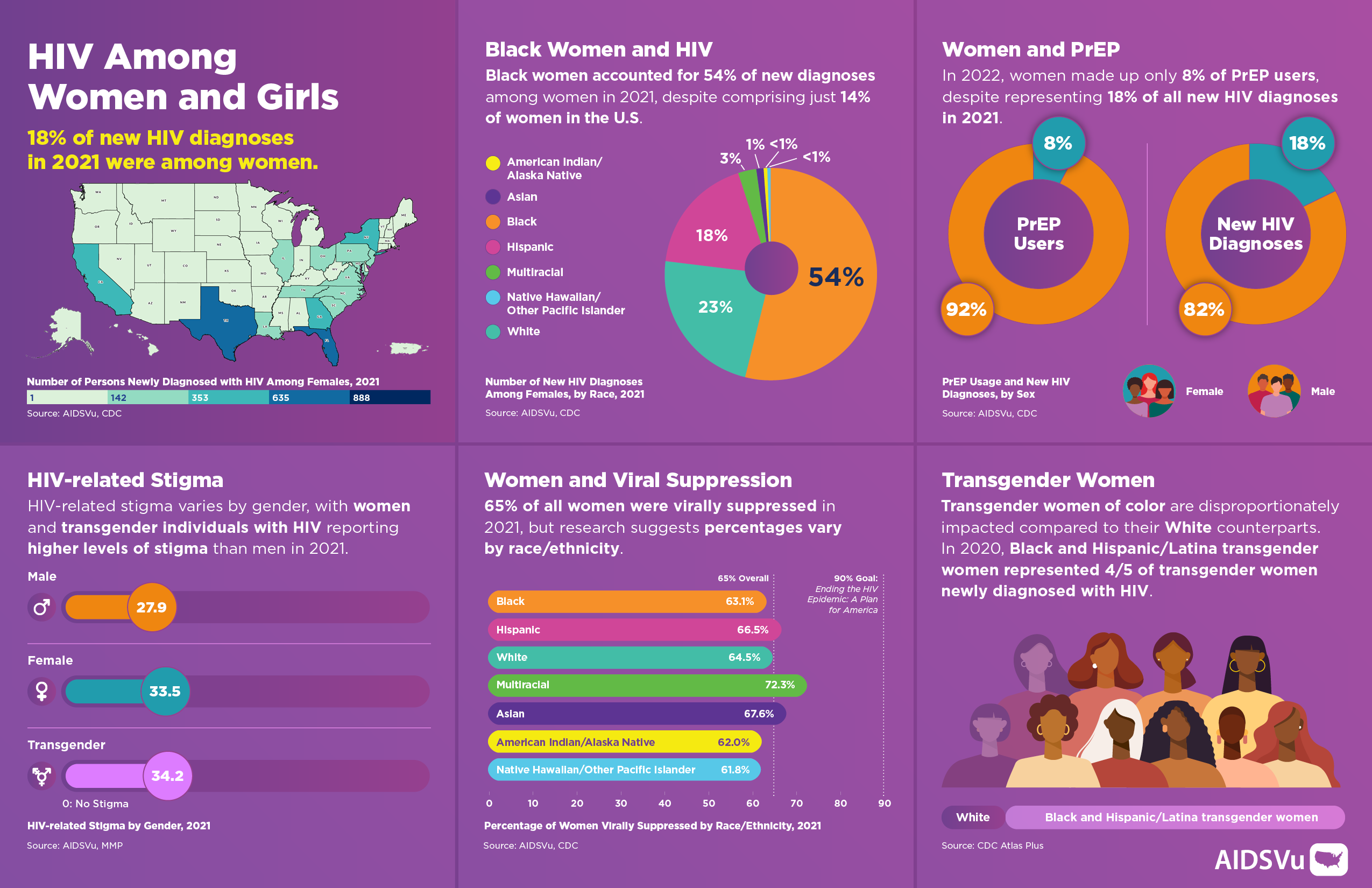
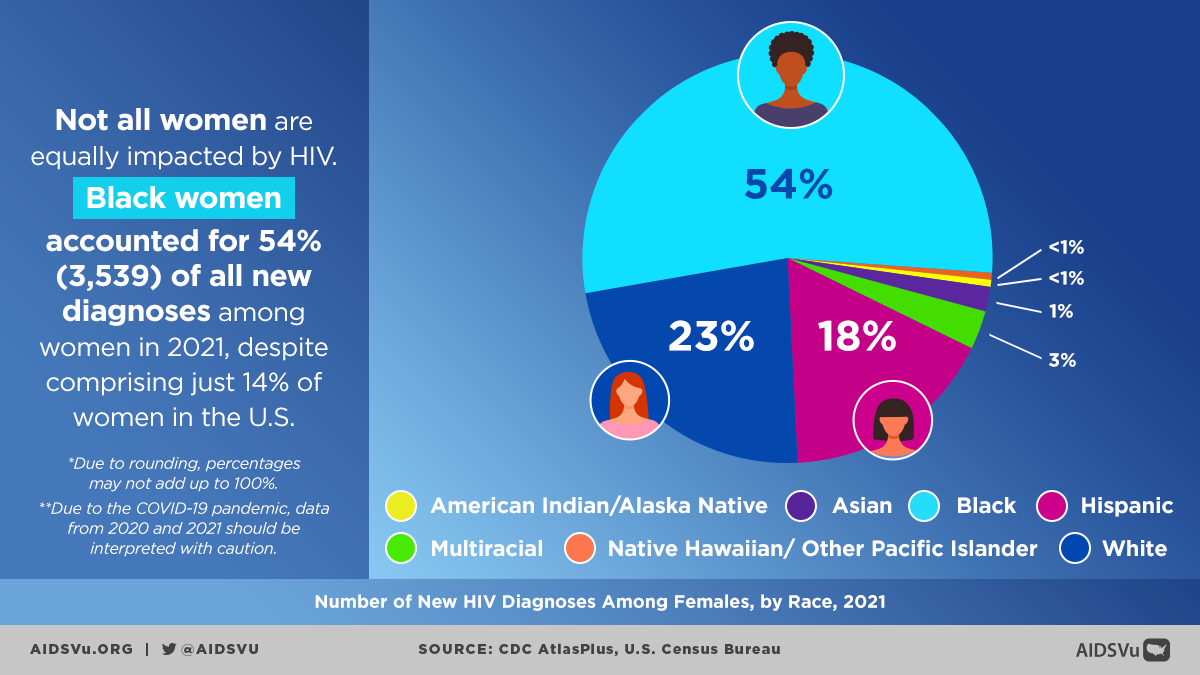
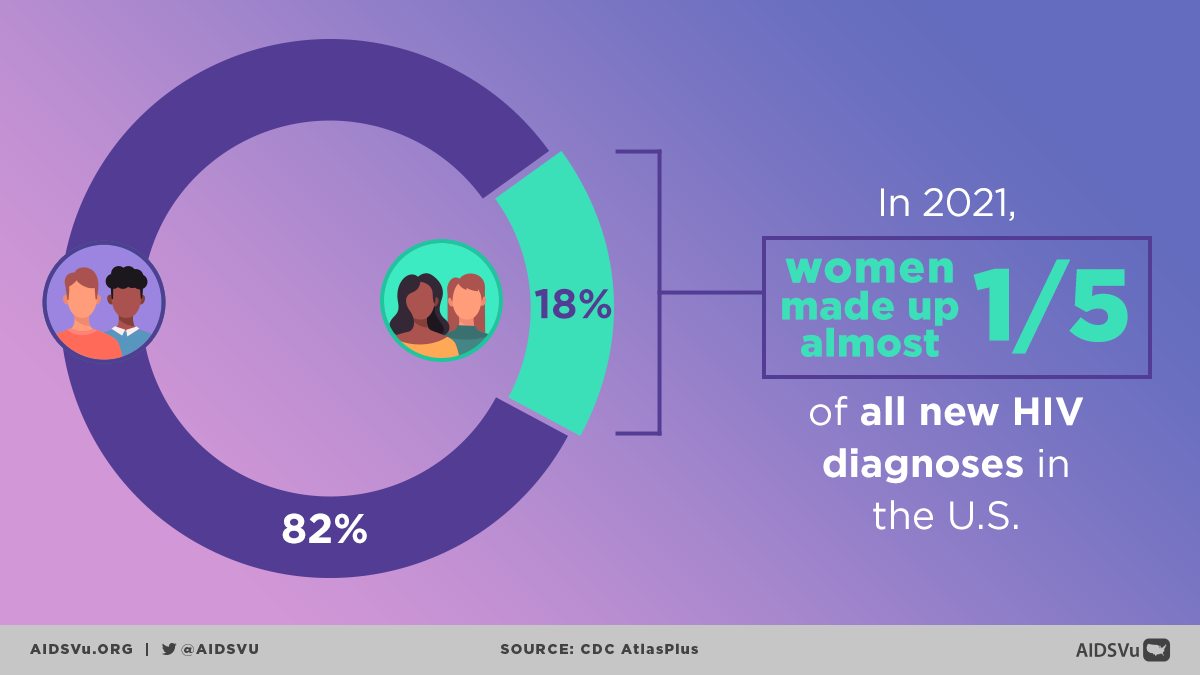
The HIV epidemic among women is heavily concentrated among Black women, who face extraordinarily high rates of infection that reflect the intersection of racism, sexism, and poverty. Black women accounted for half (50%) of HIV diagnoses among women but represent only 13% of the female population. This represents a diagnosis rate that is dramatically higher than women of other racial and ethnic groups.
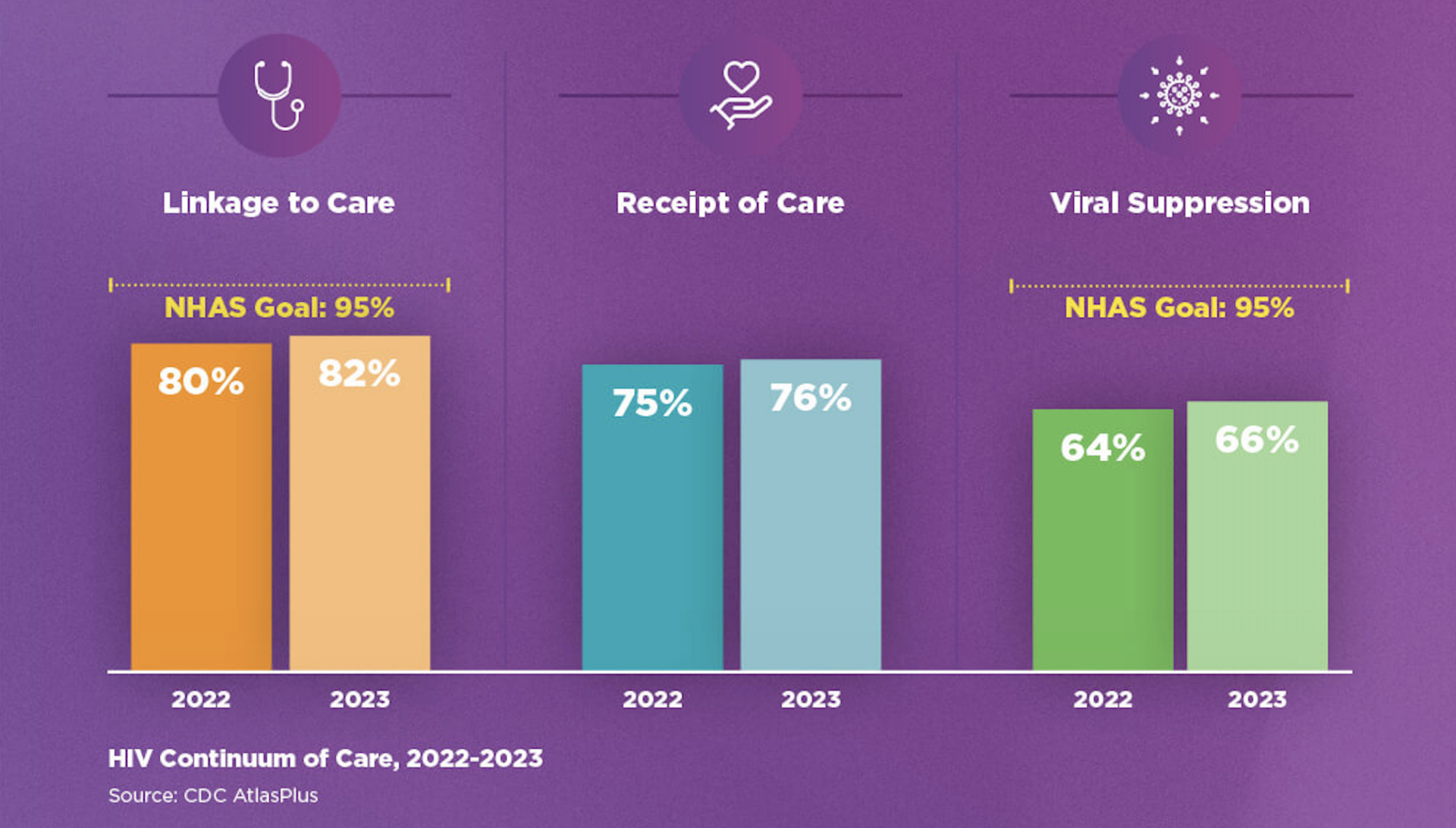
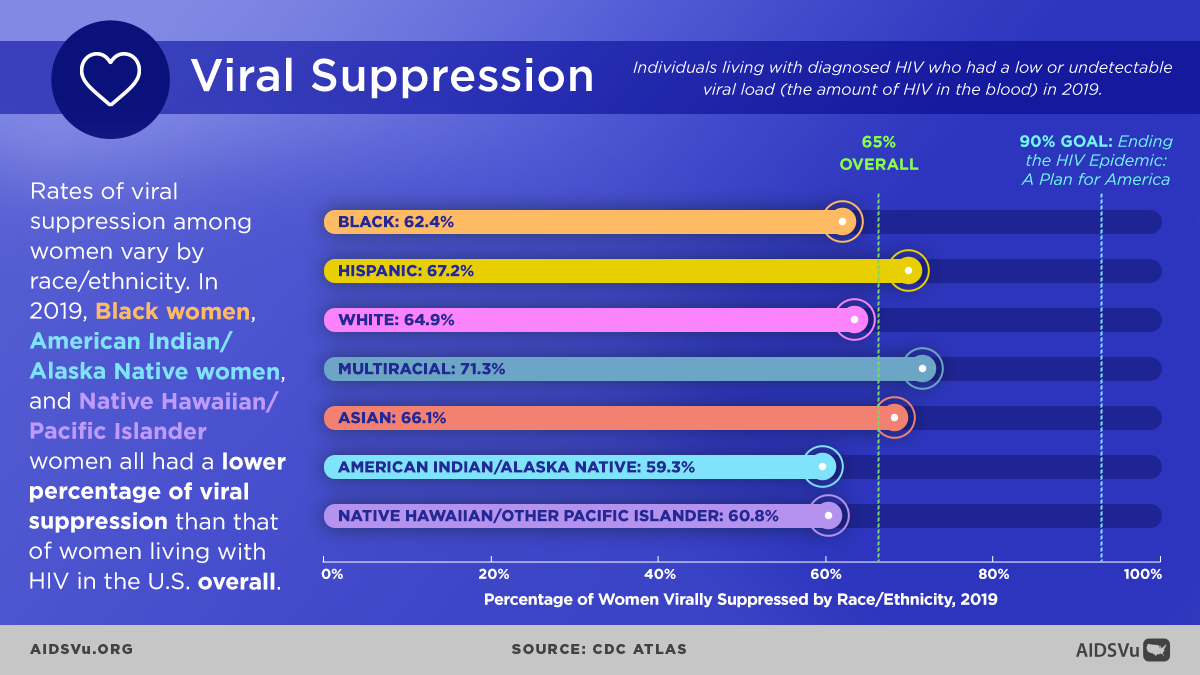
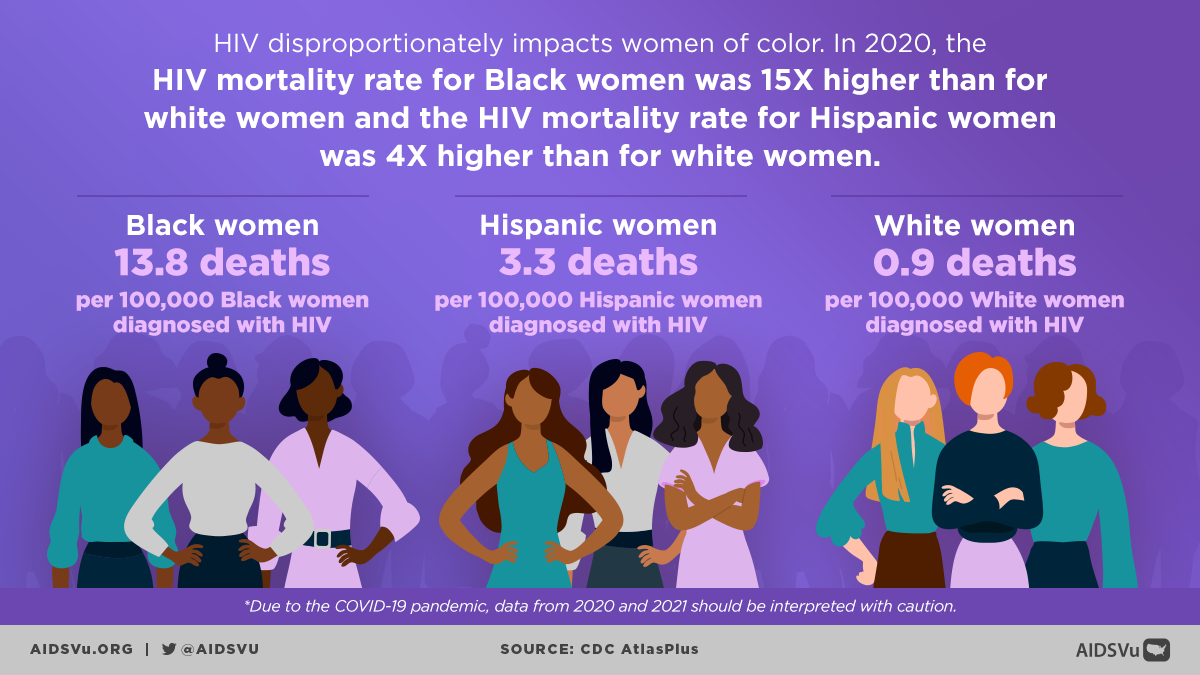
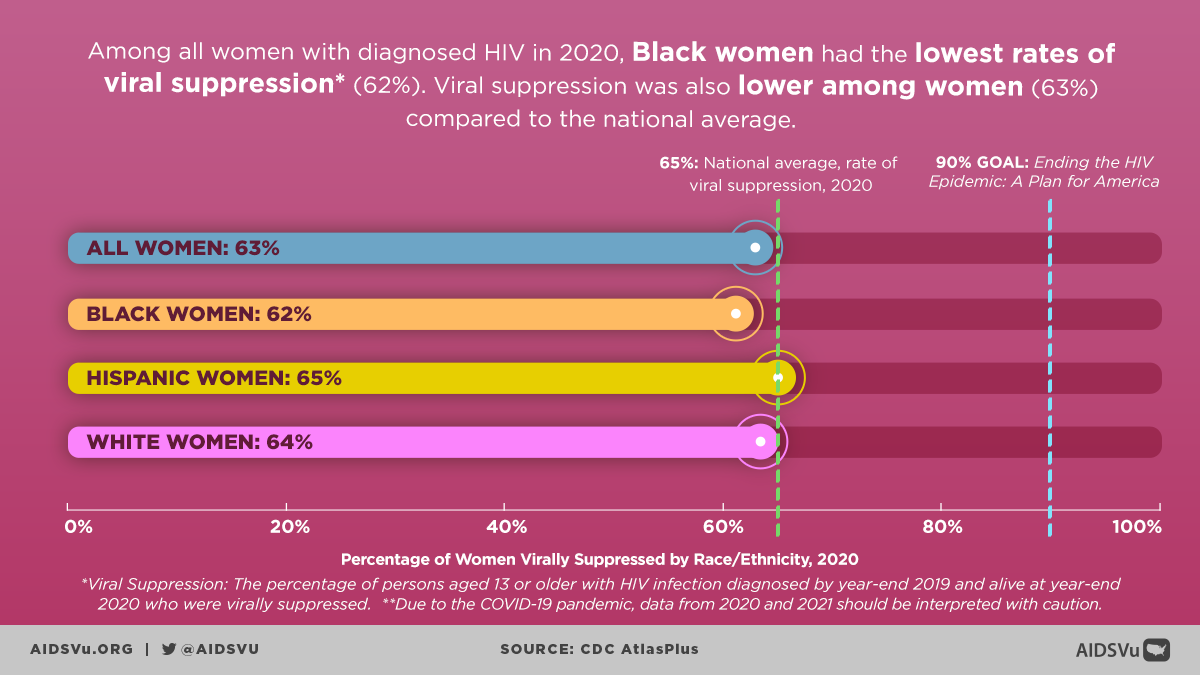
Black women had the highest HIV diagnosis rate (19.6 per 100,000), which was 3 times the rate among Hispanic/Latino women (6.7) and 11 times the rate among White women (1.8). These stark disparities reflect not individual choices but rather systematic inequities that have created conditions of vulnerability for Black women.
The Structural Roots of Disparity
The disproportionate impact of HIV on Black women cannot be understood without examining the historical and contemporary structural factors that create risk:
- Economic Inequality: Black women experience poverty at higher rates than other groups, limiting their ability to negotiate safer sexual practices, access healthcare, and leave relationships that may put them at risk.
- Geographic Concentration: Many Black women live in areas with high HIV prevalence, creating community-level factors that increase risk of exposure to HIV.
- Healthcare Barriers: Systematic racism in healthcare, limited access to quality reproductive health services, and provider bias all create barriers to HIV prevention and care for Black women.
- Mass Incarceration: The high rates of incarceration among Black men create disrupted social networks and relationships that can increase HIV transmission risk within Black communities.
- Limited Partner Options: The intersection of racism and economic marginalization can limit Black women’s pool of potential partners, potentially increasing the likelihood of relationships with men who have undisclosed HIV risk factors.


Learn From Experts
Read our series of Q&A’s with leading experts to learn more about HIV among women.









